
 ACCESS
Review Article
ACCESS
Review Article
Volume 2, Article ID: 2026.0011

Lotte Habermann-Horstmeier
Habermann-Horstmeier@viph-public-health.de

Villingen Institute of Public Health (VIPH), Klosterring 5 D-78050 Villingen-Schwenningen, Germany
Received: 24 Mar 2026 Accepted: 22 Jun 2026 Available Online: 23 Jun 2026
Background. Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a neuroimmunological disease whose diverse symptom profile is associated with dysregulation of the nervous system, the endocrine system, the immune system, and cellular energy metabolism. To date, no causal pharmacological therapy is available for this condition.
Methods. This narrative review summarizes current clinical experience from physicians, patient-reported experiences, and the results of existing studies on symptomatic therapy in ME/CFS. The latter were selected according to criteria typical of narrative reviews, namely practical relevance and feasibility.
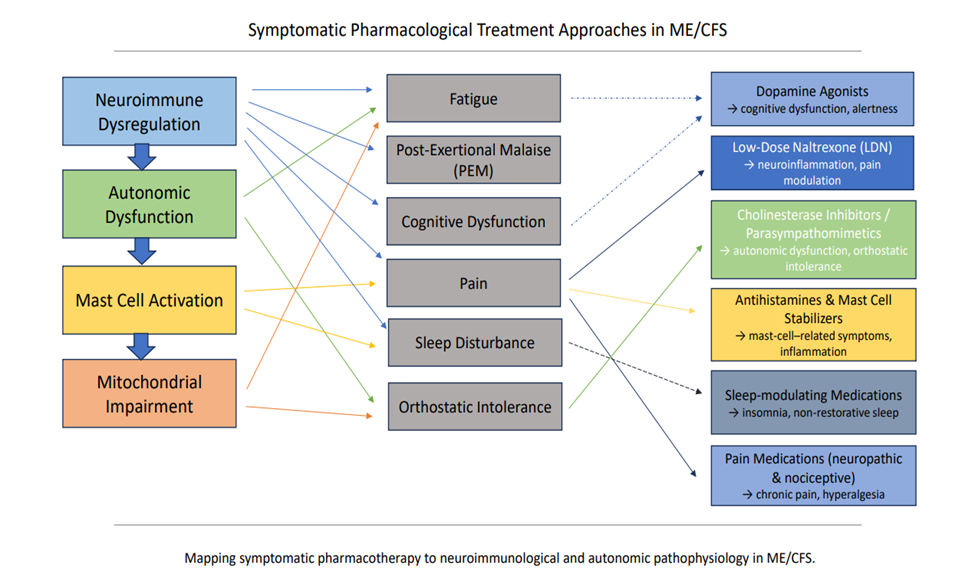
Results. Symptomatic therapy tailored to the individual ME/CFS symptom profile, in combination with consistently implemented pacing, may have a positive impact on patients’ clinical status. The medications used for this purpose are predominantly prescribed off label. Some of these drugs target the neuroimmunological pathophysiology of ME/CFS (e.g., dopamine agonists and opioid antagonists, cholinesterase inhibitors and parasympathomimetics, H1/H2 blockers and mast cell stabilizers). Others are primarily selected based on their established use in the treatment of the most common ME/CFS symptoms (e.g., quetiapine and pregabalin for sleep disturbances).
Conclusions. Since only a limited number of clinical studies have investigated the efficacy of drugs currently used in ME/CFS, comprehensive clinical trials evaluating these symptomatic therapies are needed. Beyond their therapeutic benefit, such studies could also contribute to substantiating current pathophysiological hypotheses regarding the development of individual ME/CFS symptoms.
Disclaimer: This is not the final version of the article. Changes may occur when the manuscript is published in its final format.